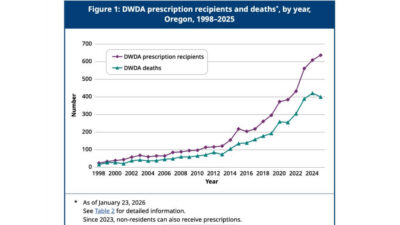
While New Zealand debates expanding euthanasia, Oregon’s latest Death with Dignity report shows prescriptions for lethal drugs reached a new record of 637 in 2025 — the highest since the law began in 1998.These latest figures show an increase of about 4.6% from the prior year, with 609 prescriptions of lethal drugs in 2024. To date, 5,520 people have been prescribed lethal drugs since Oregon’s DWDA took effect in 1997, and at least 3,691 (67%) have died after taking them, according to the OHA.
The latest annual assisted suicide report, ‘2025 Oregon Death with Dignity Act Data Summary’, released earlier this month, reveals that a total of 3,691 individuals have died by assisted suicide in Oregon since 1998. In 2025, 400 assisted suicide deaths occurred, a decrease from 421 deaths in 2024. It is likely the 400 figure will be updated, as in previous years, to include reports received after 23 January 2026. This means the final count of people who died by assisted suicide in Oregon in 20254 could be higher. For instance, in 2024, the initial report recorded 376 deaths by assisted suicide, but the mostrecent update revised this number to 421.
The report shows that, in 280 of the 400 assisted suicide deaths, there is no information on whether complications occurred. This is because data are recorded only when a healthcare provider is present at the time of death. Among the 120 cases with available complication data, seven experienced complications, such as difficulty ingesting or regurgitating the lethal substance.
According to the report, 53.5% (214) of all individuals who ended their lives by assisted suicide were female, while 46.5% (186) of them were male. What’s more alarming is that almost 2 in 5 of individuals who died by assisted suicide reported being concerned about being a burden on family, friends/caregivers.
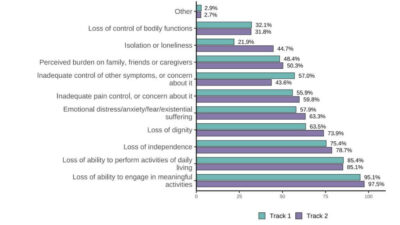
The 2025 report states that the three main reasons that Oregonians asked for assisted suicide were: 89% Losing autonomy, 89% Less able to engage in activities that make life enjoyable, 65% Loss of dignity (an undefined concern). Alarmingly, the report reveals an absence of medical oversight, with fewer than 1% of assisted suicide deaths involving a psychiatric evaluation, and in a large proportion of cases, no medical professional was present at the time of death.
Spokesperson for Right To Life UK, Catherine Robinson, said, “It is incredibly worrying that the number of assisted suicide prescriptions in Oregon hit a record high in 2025. Assisted suicide deaths may well have hit a record high, too, if the revision of data from previous years is anything to go by. This should serve as a stark warning to all those who believe that assisted suicide remains rare”.
Oregon Right to Life Executive Director Lois Anderson stated, “Once again, Oregon’s report on assisted suicide reveals a concerning increase in prescriptions for drugs that can cause death.” She added, “Last year, instead of receiving care, support, and the reassurance that their lives have inherent worth, 637 vulnerable individuals were prescribed medications meant to end their lives.” Anderson emphasised, “This is deeply upsetting and unjust. Our elderly, disabled, and those with complex medical needs deserve true dignity and compassion, demonstrated through love, care, and support that affirms life.” She concluded, “Legalised assisted suicide conveys the message that some lives are simply less valuable, which is the wrong message to send.”
Oregon’s data shows that the ‘rare and carefully controlled’ promise is not the reality. Once legalisation occurs, reporting becomes dubious, safeguards are gradually removed, and investment in palliative care and services alike is overlooked. Oregon’s 28-year experiment should be a red flag for New Zealand lawmakers. True compassion means caring for the vulnerable — not offering them lethal drugs.