NZ Herald 30 October 2020
ACT leader David Seymour thanked MPs for supporting the End of Life Choice Bill through Parliament.
He also thanked Dame Jenny Gibbs for “giving me the courage as a young MP to pursue this cause”, Brooke van Velden for her work in rallying support in Parliament for the bill, and National MP Chris Bishop.
He said New Zealand would be “a kinder, more compassionate, more humane society – what a great day to be a Kiwi”.
David Seymour hosted an event at Parliament from 1pm that heard from Shirley Seales and, via Skype from New York, Matt Vickers – the mother and widowed husband of euthanasia campaigner Lecretia Seales.
Shirley Seales gave an emotional speech acknowledging her daughter’s legacy.
“I’m sure [Lecretia] would never have imagined that she would still be acknowledged for the part she has played. She would be very humbled and I know she would want others acknowledged.”
She paid tribute to Matt Vickers, several lawyers who advocated for the cause, and MPs including Seymour, Maryan Street and Michael Laws.
She said it had been “particularly upsetting to hear lies about Lecretia throughout the campaign”.
“I have been tempted to respond, but my greatest reward will be a majority vote. We are extremely proud of Lecretia, and I’m sure she is smiling down on us all.”
Today’s result marks the end of the five-year journey for Seymour since he first put the End of Life Choice Bill in the ballot.
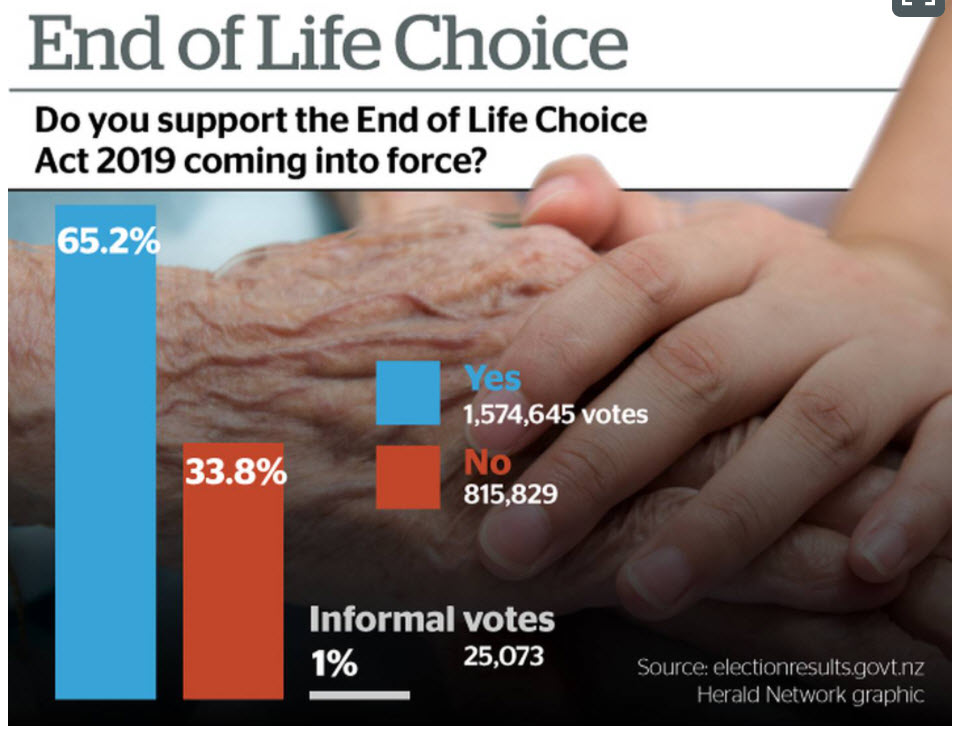
The referendum is binding and the majority “yes” vote will see it become law, with terminal patients able to request assisted dying from November 6 next year.
READ MORE: https://www.nzherald.co.nz/nz/politics/referendum-results-live-nz-votes-yes-on-euthanasia-no-on-cannabis-legalisation/LBKXYT2QB5IZLLCZJ7EVM6D4SY/
‘The devil is in the detail’: Salvation Army concerned over loopholes in euthanasia legislation
Radio NZ News 31 October 2020
Vulnerable at risk
Family First say the success of the assisted dying bill will put some vulnerable people at risk. Spokesperson Bob McCoskrie said support for the law change lowered as the debate went on.
He said many people did not realise there is an amount of choice people have in their latter days, such as turning off life support, refusing treatment, upping pain management, and do -not-resuscitate orders.
Meanwhile, a top QC said the law legalising euthanasia is shrouded in so much secrecy it will be difficult to know if anyone has been pressured into ending their life.
Auckland barrister Grant Illingworth said two doctors must sign off on someone’s request to die, but there is no requirement for them to ensure that the person has not been pressured.
“The processes under the act are shrouded in confidentiality and secrecy so nobody is ever really going to know whether people have been bullied or pressured or whether something has gone wrong in the process.
“It’s a confidential process, it’s surrounded by secrecy so how do we know?”
He said the regulations fail to require doctors to satisfy themselves there’s no coercion of a patient.
The chair of Risky Law New Zealand said the law will compromise the capacity of doctors to show undivided care and compassion to patients.
Dr Peter Thirkell said the lack of safeguards remains a big concern, particularly where patients already feel a burden to others.
The group is calling on the government to fully fund palliative and hospice services so that intentionally killing some people in vulnerable circumstances becomes unnecessary.
READ MORE: https://www.rnz.co.nz/news/national/429542/the-devil-is-in-the-detail-salvation-army-concerned-over-loopholes-in-euthanasia-legislation
Referendum results: ‘Sad and dangerous’ day, say opponents to End of Life Choice Act
Stuff co.nz 30 October 2020
Family First national director Bob McCoskrie said some would be euthanised without a definitive prognosis. Others would request “assisted suicide” as a result of coercion, or because they could not afford treatment.
“Others will be struggling because of a terminal disease prognosis and actually just need appropriate support.
“This law now means that vulnerable people facing a terminal illness will be asking themselves – why should I not be accessing euthanasia?”
Opponents to the Act said there were already calls for it to be extended from pro-euthanasia advocates.
Many New Zealanders did not understand what they were voting for, and the outcome was based on misinformation and confusion, Euthanasia-Free NZ spokesman Renee Joubert said.
Polling during the voting period showed 80 per cent of New Zealand adults misunderstood what the End of Life Choice Act would legalise.
Only 20 per cent of respondents understood the Act would not make it legal to turn off machines that were keeping people alive – that was already legal.
“It’s disappointing that the New Zealand public were generally uninformed about the details of the End of Life Choice Act.”
Joubert said the group would continue to lobby against any extension to the law.
READ MORE: https://www.stuff.co.nz/national/health/euthanasia-debate/123245906/referendum-results-sad-and-dangerous-day-say-opponents-to-end-of-life-choice-act
 Keep up with family issues in NZ.
Keep up with family issues in NZ.
Receive our weekly emails direct to your Inbox.