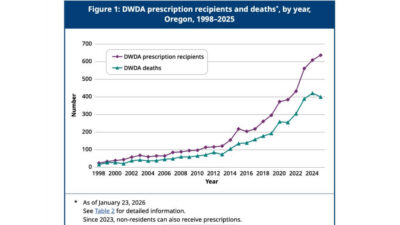
While New Zealand debates expanding euthanasia, Oregon’s latest Death with Dignity report shows prescriptions for lethal drugs reached a new record of 637 in 2025 — the highest since the law began in 1998.These latest figures show an increase of about 4.6% from the prior year, with 609 prescriptions of lethal drugs in 2024. To date, 5,520 people have been prescribed lethal drugs since Oregon’s DWDA took effect in 1997, and at least 3,691 (67%) have died after taking them, according to the OHA.
The latest annual assisted suicide report, ‘2025 Oregon Death with Dignity Act Data Summary’, released earlier this month, reveals that a total of 3,691 individuals have died by assisted suicide in Oregon since 1998. In 2025, 400 assisted suicide deaths occurred, a decrease from 421 deaths in 2024. It is likely the 400 figure will be updated, as in previous years, to include reports received after 23 January 2026. This means the final count of people who died by assisted suicide in Oregon in 20254 could be higher. For instance, in 2024, the initial report recorded 376 deaths by assisted suicide, but the mostrecent update revised this number to 421.
The report shows that, in 280 of the 400 assisted suicide deaths, there is no information on whether complications occurred. This is because data are recorded only when a healthcare provider is present at the time of death. Among the 120 cases with available complication data, seven experienced complications, such as difficulty ingesting or regurgitating the lethal substance.
According to the report, 53.5% (214) of all individuals who ended their lives by assisted suicide were female, while 46.5% (186) of them were male. What’s more alarming is that almost 2 in 5 of individuals who died by assisted suicide reported being concerned about being a burden on family, friends/caregivers.
The 2025 report states that the three main reasons that Oregonians asked for assisted suicide were: 89% Losing autonomy, 89% Less able to engage in activities that make life enjoyable, 65% Loss of dignity (an undefined concern). Alarmingly, the report reveals an absence of medical oversight, with fewer than 1% of assisted suicide deaths involving a psychiatric evaluation, and in a large proportion of cases, no medical professional was present at the time of death.
Spokesperson for Right To Life UK, Catherine Robinson, said, “It is incredibly worrying that the number of assisted suicide prescriptions in Oregon hit a record high in 2025. Assisted suicide deaths may well have hit a record high, too, if the revision of data from previous years is anything to go by. This should serve as a stark warning to all those who believe that assisted suicide remains rare”.
Oregon Right to Life Executive Director Lois Anderson stated, “Once again, Oregon’s report on assisted suicide reveals a concerning increase in prescriptions for drugs that can cause death.” She added, “Last year, instead of receiving care, support, and the reassurance that their lives have inherent worth, 637 vulnerable individuals were prescribed medications meant to end their lives.” Anderson emphasised, “This is deeply upsetting and unjust. Our elderly, disabled, and those with complex medical needs deserve true dignity and compassion, demonstrated through love, care, and support that affirms life.” She concluded, “Legalised assisted suicide conveys the message that some lives are simply less valuable, which is the wrong message to send.”
Oregon’s data shows that the ‘rare and carefully controlled’ promise is not the reality. Once legalisation occurs, reporting becomes dubious, safeguards are gradually removed, and investment in palliative care and services alike is overlooked. Oregon’s 28-year experiment should be a red flag for New Zealand lawmakers. True compassion means caring for the vulnerable — not offering them lethal drugs.
The runaway train continues. The Netherlands has released its yearly report on euthanasia, revealing that 10,341 individuals died by euthanasia in 2025 — the highest annual total since legalisation in 2002. This represents a 3.8% increasefrom 2024, with euthanasia accounting for nearly 6% of all Dutch deaths (173,314 total deaths).
One of these deaths involved a young person aged between 12 and 18. The Regional Euthanasia Review Committee report provides no further details on the case, other than confirming it was based on a physical condition rather than a psychiatric one.
According to the report, nearly three-quarters (74.7%) of individuals who received euthanasia were aged over 70. Over 85% of cases involved common physical conditions such as cancer, disorders of the nervous system, lung conditions, or cardiovascular disease. There were 174 cases involving mental health disorders as the primary ground — 45 fewer than in 2024, a decrease of approximately 21%.
Although the majority of cases involved people over 70, 33 cases concerned individuals aged 18–30, 71 cases those aged 30–40, and 160 cases those aged 40–50. The third-largest group was people aged 60–70.
Dementia-related euthanasia cases rose by 17% in 2025, while cases involving an accumulation of age-related conditions increased by 20% (from 397 in 2024 to 475). Duo-euthanasia — where two closely related people (such as partners, siblings, or parent and child) receive euthanasia together — also rose, with 60 cases recorded, an 11% increase from 2024.
The Dutch model has long been regarded internationally as an example of a balanced and careful system, even as it includes psychiatric conditions and minors. However, since legalisation in 2002, the data show a clear, long-term upward trend. The number of official notifications has increased more than 5.5-fold, rising from under 2,000 per year in the early 2000s to over 10,000 in 2025. As a share of all deaths, euthanasia has grown from roughly 1.3% to nearly 6%.
While supporters of euthanasia may point to the relatively slow growth this year and the decreasing number of psychiatric cases, the overall trajectory remains one of steady increase. An expansion that now includes young people and a persistent rise in psychiatric and dementia-related cases is not necessarily something to celebrate. As Charles Lane has argued in The Atlantic, the Dutch experience may serve as a warning that the risks of euthanasia represent less of a slippery slope and more of a runaway train.
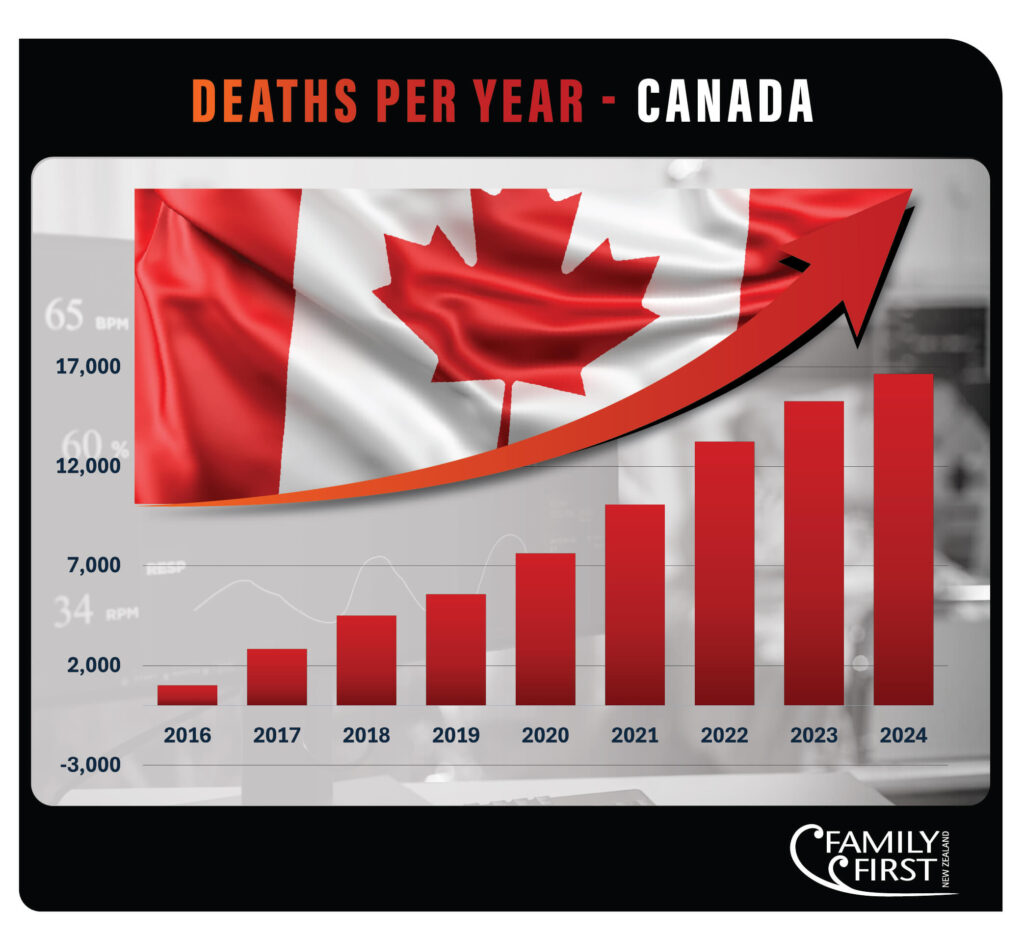
In just four years, deaths from assisted suicide/assisted dying in Alberta, Canada, increased by 109 percent. This is the reality Premier Danielle Smith’s government in Alberta faced when she introduced Bill 18, the Safeguards for Last-Resort Termination of Life Act, on 18 March 2026. It is also a reality that New Zealanders should pay close attention to, because Canada’s assisted suicide trajectory is linked to New Zealand’s story. It acts as a warning.
So what does the Bill actually do?
Restrict who qualifies – Only adults 18 and over whose natural death is likely within 12 months (Track 1) would be eligible. Track 2 MAID — for those not facing imminent death — would be banned entirely. Also prohibited: MAID for those under 18, those lacking decision-making capacity, those whose sole condition is mental illness, and advance requests.
Tighten the assessment process – Before assessing a patient, doctors and nurse practitioners must make reasonable efforts to contact every primary care provider the patient has seen in the past 12 months, and review all of the patient’s health and personal information.
Require a family witness – A family member — defined as a parent, spouse or partner, child, sibling, grandparent, or grandchild — must be present when MAID is administered, unless the provider determines one is not reasonably available.
Restrict what providers can say and do – Health professionals cannot raise MAID as an option with patients — the patient must bring it up first. Referrals out of province for MAID assessments would be banned. Public display of MAID information within healthcare facilities (such as posters) would also be prohibited.
Mandate training and enforce compliance – All MAID assessors and providers would need to meet new training requirements. Sanctions — starting with remedial training and escalating to suspension or loss of the right to provide MAID — would apply to any provider who breaches the legislation.
Protect conscientious objectors – Individual doctors and nurse practitioners would have an explicit legal right to refuse to participate in MAID. Certain facilities — including faith-based ones — would have the right to refuse MAID on their premises entirely, and could establish a 150-metre exclusion zone around their building where MAID services would not be permitted.
Should the bill pass, Alberta would become the first Canadian jurisdiction to place these kinds of limits on federally permitted assisted suicide deaths. The legislation would also proactively limit access to MAID in situations where the federal government has indicated it might implement changes.
Critics are framing this legislation as cruel because it forces suffering people to live against their will. However, supporters of the bill say otherwise.
Inclusion Alberta CEO Trish Bowman stated that MAID was sometimes causing medical systems to offer death as an alternative to supporting people with disabilities, rather than providing the necessary support for a better quality of life. She mentioned that Alberta’s limits could help save lives.
“We know it reinforces incredibly negative and dangerous stereotypes about the value and worth of the lives of people with disabilities. And so we’re very pleased to see this legislation today that serves to protect them,” Bowman said.
Krista Carr, CEO of Inclusion Canada, says she hopes other provinces follow Alberta’s example. However, she said the limits should also compel governments to invest more into programs and support that improve the quality of life for people with disabilities.
Canadian Mental Health Association research librarian Robert Olson called the legislation “heartening” and noted that their organisation opposes the expansion of MAID to people with mental illness.
Dr. Ramona Coelho, an Ontario family doctor who spoke at the bill’s introduction, has documented something deeply troubling in her practice: marginalised patients — people struggling with poverty, social isolation, inadequate housing — being offered assisted death instead of the comprehensive care that could actually ease their suffering. “Patient suffering can be addressed,” she said, “and their lives can greatly improve if we take that time.”
This is the heart of the bill. A refusal to let the medical system off the hook by offering death where it should be offering care.
Canada introduced medical assistance in dying in 2016, initially for the terminally ill only. By 2021, a court ruling expanded eligibility to include people who were not dying imminently. By 2024, Quebec began allowing advance requests — meaning people could arrange their death while still lucid, for a future date. And by March 2027, the federal government is scheduled to allow assisted suicide for people whose sole underlying condition is a mental illness.
Read that again. Mental illness. Alone. As grounds for an assisted suicide death.
New Zealand’s End of Life Choice Act came into force in November 2021, limiting assisted dying to adults with a terminal illness likely to end their life within six months. Canada started with similar bones.
Our law may be due for change. The pressure to expand eligibility to non-terminal conditions, to those suffering from psychological conditions, to younger people, will come. It always does. The Canadian experience shows us exactly where that pressure leads when it is not resisted.
Alberta’s Bill 18 is significant because it reflects a government willing to oppose and take action on the MAID programme, which has shown itself to be spiralling out of control – not just in Alberta but across Canada.
The solution to suffering isn’t a faster, cheaper, tidier way out. It is investing in palliative care, mental health services, disability support, and resources to assist families supporting loved ones through difficult times. That is the alternative Alberta’s own critics of the bill acknowledged was missing. That is what our most vulnerable truly need.
Now, the “slippery slope” in the euthanasia debate, whether here at home or internationally, was not merely a scare tactic; it functions as a roadmap, and we are witnessing it happen in real time. Perhaps, the better metaphor is that the slope is no longer slippery—it’s a cliff.
On 17 March 2026, the Scottish Parliament rejected the Assisted Dying for Terminally Ill Adults (Scotland) Bill at Stage 3, with 69 MSPs voting against, 57 voting in favour, and one abstention. The bill, introduced by Liberal Democrat MSP Liam McArthur, would have permitted terminally ill, mentally competent adults with a prognosis of six months or less to request assistance to end their lives, subject to safeguards.
In May 2025, the legislation passed Stage 1 with a vote of 70 to 56, approving its core principles. Stage 3 involved extensive debate across multiple sessions, with over 300 amendments discussed, including a late change to limit eligibility to those with a six-month prognosis.
Supporters, including McArthur and Scottish Conservative MSP Sandesh Gulhane (a practising GP who chaired the bill’s medical advisory group), argued that the bill was carefully drafted with solid safeguards. They claimed it would offer compassion and dignity to those facing terminal illness, ease severe suffering, prevent unsafe travel abroad for assisted dying, and ensure proper oversight rather than unchecked deaths.
Gulhane stated: “Choice matters. This bill represents years of work, consultation and scrutiny. It offers compassion, safeguards and dignity for those facing the end of life.”
Opponents, including disabled MSP Jeremy Balfour and some SNP and Conservative members, raised concerns about risks of coercion, especially for disabled or vulnerable people, potential pressure on individuals to avoid being a burden, and changes to the doctor-patient relationship. They argued that no safeguards could fully eliminate the risk of abuse.
Balfour, who was born without a left arm and with a shortened right arm, said disabled people felt “terrified” by the proposals and warned that the bill could open Pandora’s box with insufficient protections against coercion. “I’m begging you to consider the consequences for the most vulnerable,” he said.
Many MSPs opposing the bill emphasised the need to prioritise improvements in palliative care, social care, and protections for vulnerable groups before any change to the law.
After the vote, campaign groups on both sides issued statements. Dignity in Dying expressed disappointment but reaffirmed its commitment to pursuing reform, citing strong public support in some polls. Opponents like Right To Life UK and CARE for Scotland welcomed the result, viewing it as a safeguard for vulnerable individuals.
The bill was subject to a free (conscience) vote, with no party whips. This marks the latest in several unsuccessful attempts to introduce assisted suicide legislation in Scotland, though it progressed further than previous efforts. Attention may now (and should) shift towards improving palliative care.
A frontline New Zealand GP has exposed a troubling financial incentive at the heart of our end-of-life system — assisted dying pays up to six times more than palliative care. According to an article in Doctor NZ, Fiordland Medical Practice specialist GP Stephen Hoskin has written to Deputy Prime Minister David Seymour, raising urgent questions about why the system is structured this way, and who is responsible for fixing it.
The numbers are stark. Under his PHO, Dr Hoskin can claim $517.50 per patient for providing palliative care in the community. This covers every visit, every call, every hour spent supporting a dying person and their family. By contrast, the Te Whatu Ora website indicates a GP could claim up to $3,080 for a single assisted death. This isn’t a technical error either. This is a system that has been built (unintentionally or not) to reward ending lives over supporting them.
This isn’t a claim from a lobby group. It’s the assessment of a working rural doctor. Dr Hoskin describes the situation as “deeply concerning and unethical,” warning that even well-meaning doctors carry unconscious biases. When a patient raises assisted dying, and a doctor knows they could earn six times more by proceeding rather than redirecting towards palliative care, can we truly say that the consultation is unbiased? Dr Hoskin doesn’t think so, and neither should we.
The rural health disparities make this worse. Some palliative care visits in rural New Zealand are reimbursed at under $50 — less than the cost of a standard GP consultation, and a fraction of what urban patients may receive. Why doesn’t a dying person in Fiordland deserve the same quality of end-of-life support as someone in Wellington? Despite the Government spending $119 million on hospice care for 2025/26, these disparities persist.
Before the End of Life Choice Act was passed, and again during its three-year review, pro-life advocates and organisations, including Family First NZ, warned that financial disparities and perverse incentives would follow. Those concerns were dismissed as scaremongering. Well, it looks like this recent exposure by Dr Hoskin confirms what we have always said — the system is not neutral. It structurally incentivises death over palliative care, and it has been doing so since the Act came into force in November 2021.
And it appears from the deflection in responses from Seymour to the Health Minister to Te Whatu Ora, no one is taking accountability for a system that Dr. Hoskin describes as “deeply concerning and unethical. While Te Whatu Ora recognises that palliative care funding is “inconsistent across New Zealand” and mentions a National Palliative Care Work Programme but provides no timeline or specific commitments.
Three deflections. Zero answers. Nobody owns this.
And the push to expand the system continues regardless. A proposed amendment bill, lodged by ACT’s Todd Stephenson, wants to make it easier for doctors to raise assisted dying directly with patients — removing one of the few remaining safeguards in the current legislation. Even more troubling, the bill includes removing the 6-month prognosis time-limit and looks to pressure palliative care facilities to participate in assisted dying services. Organisations built around the sanctity of life and caring for the dying could be compelled to facilitate death instead. Combined with the financial incentives already baked into the system, this expansion should alarm every New Zealander who cares about protecting the elderly, the vulnerable, and the dying.
A society’s priorities are revealed by what it funds. Right now, New Zealand is paying more to end lives than to cherish them.
Source: New Zealand Doctor Rata Aotearoa. All quotes and figures cited are drawn from their original reporting.
Yesterday, the French National Assembly voted on passing a bill legalising assisted dying. This marks the next phase in a year-long debate on euthanasia and assisted dying. The National Assembly voted in favour of the bill to legalise assisted dying in May 2025, but the French Senate rejected it and sent it back for further reconsideration about eight months later. Iterations to the bill have been made since, with the debate returning to the French parliament earlier in Jan, and a final vote held on Feb 25th. The final vote on the bill was 299 in favour and 226 against, with an absolute majority set at 263. Ironically, the accompanying bill on palliative care was also unanimously passed at the same time.
With steps closer to legalising assisted dying, the euthanasia bill adopts the assisted dying model, making self-administration of the lethal substance the rule and assistance from a third party the exception if the individual is unable to self-administer. This would only be available to those who meet strict eligibility criteria, which require them to be over 18 years of age, residing in France, and suffering from a life-threatening incurable illness in a terminal stage. Individuals will also need to express their wish to end their lives. If this sounds familiar, that’s because we’ve seen the same course of action here at home.
Currently, the Léonetti Law of 2005 regulates end-of-life care, permitting individuals to refuse “futile medical care” and to access palliative treatment. In 2016, the Claeys-Léonetti Law expanded these provisions, allowing deep and continuous sedation until death under specific conditions, applicable when the patient suffers unbearably and death is deemed inevitable and imminent.
Olivier de Margerie, the president of Accompanying Life Until Death, is concerned that presenting assisted suicide as an individual liberty risks pressuring people with terminal illnesses. Mr. de Margerie argues that:
“introducing the possibility of ending one’s existence — where society organises and facilitates the process — is a direction that will, in the fairly short term, lead to a reduction in the financial, political and technical efforts to develop palliative care that is available everywhere and accessible to everyone in France.”
He’s right. Once the state normalises assisted suicide and society accepts it as normal and routine healthcare, investment in compassionate alternatives inevitably declines.
Australian bioethicist and author Xavier Symons also cautions that lawmakers in different countries considering euthanasia might underestimate how eligibility criteria could broaden over time. He notes:
“The biggest risk is establishing a ‘right to die’ that could extend far beyond terminal illness, thus allowing access to euthanasia to any group that wants it,” he said. “This includes people with mental illness, people with chronic illnesses, and even people tired of life. If it is claimed that some people have the right to euthanasia, it is difficult to deny the conclusion that all people have the right to euthanasia.”
And this is the exact pattern we are seeing in different jurisdictions like France’s neighbours, the Netherlands and Belgium, and let’s not forget Canada, where assisted suicide (they call it medical assistance in dying) is the 5thleading cause of Canadian deaths. Not forgetting that each of these countries often begins with restrictions on assisted suicide, only for expansion to follow slowly and quite drastically.
Now, whilst the French National Assembly just passed the bill again, overriding the Senate’s earlier rejection and sending it back to the Senate, which is largely conservative. But the pressure to adopt euthanasia is intensifying, and France is yet another nation on the brink of institutionalising and normalising the idea that the sanctity of life only matters for some and not others.
France’s debate will be a crucial one to follow. It highlights how rapidly a society can move from defending life to enabling death—and underscores the importance of consistently advocating for genuine compassion, true dignity, and quality palliative care, rather than state-approved killing.
ACT wants to expand euthanasia but this would breach fundamental human rights in the New Zealand Bill of Rights Act.
“ACT’s changes breach human rights and take away freedom of choice,” says Alex Penk, author of a new report for MPs on the End of Life Choice Amendment Bill. “The Bill would stop doctors and care facilities like hospices from using their conscience and making ethical decisions like they do now.”
“Assisted dying is already highly controversial and most doctors don’t want to be involved,” says Penk. “The Bill would introduce euthanasia for long-term conditions and disabilities, like chronic heart conditions, frailty, diabetes, renal failure, multiple sclerosis, and motor neurone disease. This would force doctors and care facilities into more conscience conflicts. Doctors have to use ethical judgment all the time but the Bill sends a message that they’re just supposed to do what the state tells them. There’s a real risk it’ll force ethically-minded people out of medicine.”
“ACT’s bill would also undermine palliative care. It would cover ‘care facilities’, including hospices, disability support facilities, and rest homes. Care facilities would have to be prepared to allow assisted dying even when that goes against their beliefs. Facilities like hospices do an incredible job for vulnerable people but they’re over-stretched and under-funded. They shouldn’t be backed into a corner if they don’t want to be involved in euthanising their residents.”
“This is not what Kiwis voted for,” says Mr Penk. “David Seymour said that conscience is a cornerstone of the law, and 65 percent of voters supported that law in a referendum. There is no mandate to change such a fundamental part of the law. Let individual doctors and care facilities decide if they want to offer assisted dying, or the government could just do a better job of providing information.”
“It’s ironic that a law about end-of-life choice would limit freedom of choice,” says Penk. “MPs will get a conscience vote if the Bill goes before Parliament. Why shouldn’t doctors and care facilities get to use their conscience too?”
In an opinion piece (in response to a Stuff NZ article on organ donations and assisted dying), Dr John Kleinsman of the Nathaniel Centre for Bioethics argues against combining organ donation with assisted dying in New Zealand, despite organ shortages. He highlights concerns around coercion, emphasizing the societal pressure that could make vulnerable people feel compelled to choose assisted dying or face societal expectations.
While doctors can legally refuse to participate in assisted dying, those on organ retrieval teams are inevitably connected to the process of ending life. He points out that, although the public might see ending a patient’s life and organ retrieval as separate, in practice, the medical teams must work closely together. Essentially, the organ retrieval team, whether they consent or not, will play a role in how the patient dies, making them inherently connected with the act of directly, intentionally, and prematurely ending a patient’s life. This threatens the conscientious objection rights of doctors who entered medicine to save lives, not end them, and may even exclude doctors from minority ethnic or religious backgrounds who are uncomfortable with assisted dying.
Organ recipients won’t be told if their donor died through assisted dying, which violates their autonomy. Dr Kleinsman notes that 35% of New Zealanders opposed assisted dying in the 2020 referendum, making transparency about donor circumstances crucial for respecting recipients’ right to make informed decisions.
Dr Kleinsman argues that while organ donation is normally a generous gift, the utilitarian argument of increasing organ supply by the likes of Organ Donation New Zealand (ODNZ) isn’t a sufficient justification when weighed against these ethical concerns.
*Written by Family First staff writers*
Please see here for the original article and Dr Kleinsman’s full response.
Check out our Family Matters episode with Dr. John Kleinsman
The report indicates that cancer, especially lung, colorectal, pancreatic and blood cancer, was the most frequently reported condition in nearly all age groups of people who died by MAID in 2024, except those 85 and older, “for whom ‘other’ conditions were the most frequently cited.
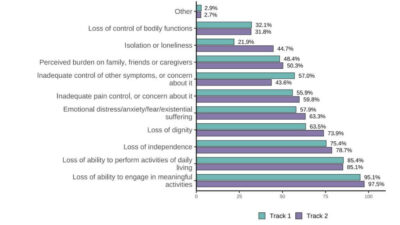
Interestingly, inadequate pain control was only the sixth most common reason for seeking MAID. The primary reasons for euthanasia deaths were related to autonomy and daily function:
Loss of ability to engage in meaningful activities (the highest reason, over 95% for both tracks).
Loss of ability to perform activities of daily living.
Loss of independence and loss of dignity
Figure: Reported nature of suffering, by track
Source: Sixth annual report: Medical assistance in dying Canada
In terms of MAID deaths across districts, Quebec has the highest number of euthanasia deaths at 5,998. MAID deaths remain heavily concentrated in three provinces, which accounted for nearly 85% of all provisions: Quebec (36.4%), Ontario (4,944 deaths, 30.0%) and British Columbia (2997 deaths, 18.2%).
Nearly all MAID deaths were performed by a doctor or nurse practitioner. While the law allows patients to self-administer the medication in most parts of the country (except Quebec), this option is rarely chosen. The typical (median) age of a person receiving MAID in 2024 was about 78 years old. Recipients who were near the end of their lives (Track 1) had a median age of 78.0 years, while those whose death was not immediately foreseeable (Track 2) were slightly younger, with a median age of 75.9 years. Overall, the average age of MAID recipients continues to rise slightly each year.
There was a notable increase in track 2 euthanasia deaths, which increased by 17% accounting for 4.4% of total euthanasia deaths and up from 4.1% in 2023. Track 2 euthanasia deaths refer to not immediately foreseeable deaths of people and are more likely not to have a terminal condition, to be women, younger and living with a disability.
Dissecting Track 2 euthanasia deaths a little further, it appears people who die by Track 2 euthanasia deaths are significantly more likely to be poor, live in institutions or poor neighborhoods, and be receiving disability support services than those who die under Track 1. Of the 16,104 people who responded to questions around disabilities, roughly one-third (32.9 per cent) reported having a disability.
Alex Schadenberg, chair of the Euthanasia Prevention Coalition (EPC), suggests that MAID for non-terminal conditions mainly targets individuals with disabilities, noting a clear link between disability and Track 2 deaths, as 61.5% of Track 2 recipients identify as disabled.
If that isn’t shocking enough, loneliness and isolation were reported as a factor in 44.7% of Track 2 deaths and 21.9% of Track 1 deaths, suggesting that over 3,800 people listed this as a primary reason. Track 2 recipients were far more likely to be receiving mental health/social support services (31.4%) compared to Track 1 recipients (9.4%), indicating that mental health is a prevalent factor in non-terminal MAID cases.
These statistics are both disturbing and tragic, highlighting pro-life advocates’ concerns about expanding Canadian euthanasia laws to include non-terminal individuals. These vulnerable groups are often affected by factors such as lower socioeconomic status, disabilities, and insufficient social support. The recent MAID data confirms this, showing that social and systemic problems—like loneliness and inadequate disability support—are significant factors influencing requests for MAID.
The most concerning finding in the 2024 Annual Report is not only the total number of MAID deaths but also the speed at which this peak was reached. Despite the growth rate slowing to 6.9% in 2024, this follows years of swift expansion that propelled Canada from having a recently legalized system to becoming a global leader in euthanasia deaths. This trend confirms that MAID is shifting from a last-resort service to a major—and quickly becoming a leading cause of death in Canada.
This week I found myself up at 4am to speak to the House of Lords in the United Kingdom. As you may know, they are considering yet another euthanasia/assisted suicide Bill and the Lords are currently holding committee hearings and wanted to know of the New Zealand experience.
There were four of us in total, two supporting life and palliative care and two that either support or lean in support of euthanasia. I was there alongside Professor Sinead Donnelly, a professor and palliative medicine physician. Naturally, I’m with Family First, but I was also there, having chaired the health committee in parliament when it then undertook the largest ever inquiry, that into euthanasia.
I will admit, it was both a very early and long morning. The way the House of Lords operates means that just about every vote requires the Lords to be there in person, so bells would ring during the hearing, and they would have to leave!
My message to the Lords was simple – euthanasia laws inevitably expand. There was a sense from some of the Lords (those in support of euthanasia) that their UK law would be exceptional, that, unlike other countries, their proposed law would be complete and never need to be changed.
I simply pointed out that every jurisdiction that introduces euthanasia laws sees expansion. I pointed out that we are only three years in here in New Zealand, and already, there is a big push to expand the law. To remove conscience rights from doctors, nurses, and hospices; to let doctors promote euthanasia to patients; for the Ministry of Health to advertise euthanasia; and to remove the likely 6 months to live requirement.
The key dynamic in play, that I attempted to succinctly explain to the Lords, was the euthanasia moves swiftly from being a health issue to a justice issue. Debate begins around terrible medical conditions (think neurological disorders such as Huntington’s disease) but swiftly moves to one about rights, not discriminating, and equal access.
I was also at pains to point out the contradictory statements being made by the New Zealand pro-euthanasia witnesses. On one hand, they were saying New Zealand’s law has important safeguards yet the very next minute they were saying that safeguards are an obstruction and prohibition that should be removed. Quite extraordinary!
A particularly memorable moment, which elicited loud gasps from the Lords present, was when one of the pro-euthanasia researchers here in New Zealand stated:
“The concerns about palliative care being undermined are more about the palliative care professionals who cannot sit with their own discomfort about assisted dying”
You can appreciate why there were gasps to this dismissive and dangerous statement. What was being strongly stated is that any moral or ethical concerns around terminating people should be put aside; that palliative care practitioners with concerns should be dismissed. This New Zealand researcher also appears blind to why people might experience such discomfort, and doubly so when it’s those in palliative care who spend their lives trying to help the dying live well to the very end.
Let’s hope that the Lords see the value of life and vote no to this proposed law.
The inevitable has happened, with the ACT Party and other pro-euthanasia/assisted suicide proponents calling for the expansion of the system. Euthanasia has been legal for barely three years, and over 1200 Kiwis have ended their lives, and already proponents want more.
We were also told that the system would be safe. It is not. As I write, we know of a tragic case where a non-English speaking woman with dementia was euthanised, despite no translator being present. There is also at least one euthanasia case now before the police.
Those put in charge of reviewing euthanasia cases noted that forms were not poorly filled out, and that what doctors were saying about their patients did not match what was written on the forms. These reviewers also questioned the lack of information provided to them, and ultimately, as these reviewers asked more questions – and became whistleblowers – they had their roles cancelled (ironically, by the author of the End of Life Choice Act and now government Minister, David Seymour).
We also know that Health New Zealand cannot even give New Zealanders accurate numbers of deaths. Its reports frequently get numbers wrong, in one instance, missing nearly half the number of people who died in one quarter.
All this to say, the current system is not working well, and mistakes are happening.
We also know that very few doctors and nurse practitioners want to be part of the service. Around 120 are involved, from a pool of 20,000. The response by euthanasia proponents and Todd Stephenson is to remove conscience rights of doctors and nurses to object. You have read that right – a law based on autonomy wants to remove autonomy from medical professionals. The same is true for hospices, with the proposed amendment wanting to force their facilities to allow euthanasia, even though it is the antithesis of palliative care. Autonomy for some, coercion for others!
We also have recent research from Auckland University that noted the main reason people seek euthanasia is fear of losing control of their lives. While clearly underlying health issues, it was people’s fear of future suffering and death that drove the requests. This was further emphasised by the doctors who noted that the ‘unbearable suffering’ criteria is totally subjective.
The same research also, distressingly, highlighted the experience of one doctor being surprised when a patient did not die quickly and instead gagged, choked, and struggled to breathe after orally ingesting lethal drugs.
Despite the rhetoric of a peaceful death, it is not always the case. Just like the reporting mistakes, the inability to objectively identify suffering, and the already simple processes being ignored, Todd Stephenson and others are pushing for an expansion.
They point to Canada, and yet this country’s approach to euthanasia should be a warning. Euthanasia in Canada is now the 5th leading cause of death, alongside the likes of cerebrovascular diseases (think the likes of strokes) and chronic lower respiratory diseases (think the likes of emphysema and chronic bronchitis). One in twenty, or 5%, of Canadians now die by euthanasia. Euthanasia was billed as something rare, and proponents continue to provide the ‘next hard case, ’ but it is clear it expands and expands. Sticking with Canada, they have even changed the law to allow mental illnesses (though it is yet to take effect) and are discussing euthanising babies and children.
A final observation. Proponents of euthanasia continue to couch their language in terms of compassion and love. Let’s be clear, euthanasia and assisted suicide have nothing to do with ‘compassion’ or love. Quite the opposite. Compassion literally means to suffer with; it does not mean to eliminate the sufferer (which ironically, is more often those watching a loved one die, not the loved one). And love seeks to provide hope and care, not removal.
As state-assisted suicide is normalised, international evidence reveals a disturbing trend.
Of a total of 252 jurisdictions worldwide, only 24 allow some combination of euthanasia and assisted dying. These jurisdictions are the Netherlands, Switzerland, Belgium, Luxembourg, Colombia, Canada, Portugal, Germany, New Zealand; the US states of Oregon, Montana, Washington, Vermont, California, Hawaii, New Jersey, Maine, and the District of Columbia; the Australian states of Victoria, Western Australia, Tasmania,
New South Wales, Queensland and South Australia.
This means that euthanasia or assisted dying is legal in only about 10% of jurisdictions worldwide.
In this latest Fact Sheet we publish our findings for Canada, Netherlands, Belgium, the US state of Oregon, and Victoria Australia, and of course New Zealand.
Euthanasia in New Zealand
In New Zealand, in just three years, we have already had over one thousand people terminate their life early. This is far more than the ‘tens’ a year that were suggested by pro-euthanasia advocates when arguing for a law change.
We are also hearing calls – as has happened overseas – to
expand the law. This includes:
widening what medical conditions are included (beyond just terminal diseases)
how long before you are expected to die (to extend beyond six months)
removing a protective requirement that limits the ability of medical professionals to publicly discuss euthanasia so that medical professionals can raise the option of euthanasia
removal of conscientious objection from medical & health professionals as well as facilities like hospices, plus discussions about allowing eligibility for mental illness.
There is concrete evidence from the countries which have introduced euthanasia that the availability and application of euthanasia expands to situations not initially envisaged.
When a newly-permitted activity is characterised as a ‘human right’, the overseas experience is that there is an inevitable push to extend such a ‘right’ to a greater number of people, such as those with chronic conditions, disabilities, mental illness, those simply ‘tired of life’, or even children.
There’s also the elephant in the room. The End of Life Choice Act only provides a ‘right’ to one choice – premature death. There is no corresponding right to palliative care. Good palliative care and hospice services are resource intensive; euthanasia would be cheaper.
There is a new element of ‘financial calculation’ into decisions about end-of-life care. This is a harsh reality.
At an individual level, the economically disadvantaged who don’t have access to better healthcare could feel pressured to end their lives because of the cost factor or because other better choices are not available to them.
Conclusion
One of our concerns expressed during the recent euthanasia debate and referendum was the reality that terminally ill people are vulnerable to direct and indirect pressure from family, caregivers and medical professionals, as well as self-imposed pressure.
They may come to feel euthanasia would be ‘the right thing to do’; they’ve ‘had a good innings’; or do not want to be a ‘burden’ to their nearest and dearest. It is virtually impossible to detect subtle emotional coercion, let alone overt coercion, at the best of times.
Because we’ve legalised it, we’ve normalised it.
No longer is the option of euthanasia ‘off the table’ in New Zealand. It’s clearly on the table and being served up to look like a fine meal, when in reality, it is just about bringing about premature death and putting the vulnerable at greater risk. Similar to the slippery slope trends we see unfolding overseas, there are more attempts here in New Zealand to expand the End of Life Choice Act. This will allow even more vulnerable people to qualify for the state to help end their lives.
The latest review of euthanasia has just been released by the Ministry of Health – and despite a tiny workforce, there has been a continued growth in the number of those receiving assisted suicide.
Family First is appalled to see that the Ministry of Health has once again erroneously reported euthanasia numbers in New Zealand including one quarter where the number of deaths nearly doubled.
The Maxim Institute’s Research Manager, Maryanne Spurdle, joins Simon to discuss her latest research – Interrogating Choice: Euthanasia and the illusion of autonomy. Simon and Maryanne discuss how the underfunding of palliative care is removing genuine choices from individuals at the end of life. They also talk about the increased push by the likes of the Ministry of Health and others to remove doctors, nurses, and hospices’ conscience rights – that is, force people to participate in something they do not want too.
Simon: Hi everyone. Great to have you back here on The Family Matters podcast. As I always say, we are going all around the world, but we’re back in New Zealand this week. I’m very pleased to bring back on to the podcast Marian Spurtle, she’s now the research manager at the Maxim Institute has been part of the research team, but now we are managing it Maryanne.
So congratulations on that.
Maryanne: Oh, thank you. Good to be with you.
Simon: Well, good to have you back. Last time we were talking education this time we are, we’re still speaking in a space beginning with e but a heavier topic particularly around euthanasia, but broader than that conscience rights autonomy freedom, palliative care and so on.
But the reason is because you’ve just released a discussion paper called Interrogating Choice Euthanasia. And the illusion of autonomy hence bringing you on the show. So give us a quick introduction for those who, well, first and foremost, they should go onto the Maxim website and read it. It’s only 23 pages.
And can I say easy to read but give viewers a bit of a sense of what this paper’s about.
Maryanne: Yep. Well, as we’re all aware now, euthanasia is legal. It has been frigid over three years, and the Ministry of Health, one of the requirements of the law is that after it was in effect for three years, they had to do a survey of how it was going and publish a report.
So that came out last November, and it was interesting reading. If you take it at face value, it’s saying the legislation is working fine. We just have a few little glitches to work out. But when you look into the problems with how it’s being well, I mean the, there are problems with. The fact that there’s now a legal way to kill people, that immediately brings up challenges, but the actual way it’s being implemented doesn’t match the way it is on paper.
So on paper there’s a review committee that checks things after they’ve happened and make sure that yep, ev everything is aligning with the legislation. Before the review even came out, two of the former reviewers publicly expressed concerns. So I’ll go into a little bit of that. That’s in the paper.
So it’s not even lining up with the legislation. And now we’ve got the Ministry of Health Review. It’s suggesting some changes, some of which are to close gaps but most of which are to expand access, make access easier for people who want to and the trouble is that’s an intention with safety.
As soon as you make something. Easier to access, you make it less safe when it’s something that, that has risks like coercion. So my paper is looking at first of all, what in the legislation is problematic because it’s called End of Life Choice Act. How good is the choice it offers? And then given the ministry’s view of how it’s been implemented and what, what should change?
Does that actually assist choice or does it limit choices for people de despite what it says in you know, face value, the word is choice, but is it,
Simon: which, you know, spoiler alert from my side what they’re suggesting, and I think what you will not think, I know what your papers said is actually going to limit.
Choice. In fact, one thing that struck me amongst many you discussed well, one of the recommendations or suggestions put to the ministry and the review was to have this cooling off period to give people a little bit more time to ponder the early termination of their life. And the ministry ultimately said, no.
We understand it will make things safer but it won’t facilitate access. This equity of access just kept coming on through. So in many ways that they’re happy to. Reduce that choice decrease safety, just to make this more, I think you used the word somewhere in the port to normalize euthanasia, and that struck me as something in their review.
Maryanne they very much want to normalize.
Maryanne: That’s their words as well, not mine. Yeah.
Simon: Oh yeah. I should, yeah. Should be yes, we should be accurate about that. Maryanne’s,
Maryanne: I’m using that word, but yeah, they are trying to normalize it, but they’re even saying, they’re trying to normalize it. This isn’t, if you know.
Don’t access it if you don’t want it, it’s there if you can. This is, everyone should be accepting this. And it, we get into freedom of conscience issues because of course, euthanasia is not isolated to that individual because it involves health practitioners. And if a person is living in a care home, it has implications for the care home for hospices, it has implication for hospices.
So this isn’t. You are an individual. If you wanna choose that, great. Go for it. It’s not gonna impact anyone else. This is quite different. It is. This is something that other people are impacted by.
Simon: It is certainly, one of the things I’ve often argued in the autonomy space, and you’ve just echoed it, is the person making the decision is never doing it alone, as you said, from the medical to the health practitioners, hospices, hospitals private, well, even some private facilities, but also the wider family.
There’s always a lot of other people impacting and coercion is one of the areas you touch on in your discussion paper as well. But let’s just tease some of that out, starting around. Conscience rights because one of the more disturbing elements for me coming out of the ministry’s review and what you address in your discussion paper, is the ministry wanting to remove conscience rights from individuals.
So thinking doctors and nurses, and they’re wanting to remove conscientious rights from the likes of hospices or entities. I mean, what is driving that you think from the ministry side?
Maryanne: This is not limited to the Ministry of Health here. This is an international issue. So conscientious objection is something that doctors are able to do legally.
So you, you cannot force someone to participate in something if there is a conscientious objection, right? And for both abortion and euthanasia, those are two things within the health system that there are those rights for. Other countries have these rights in Canada, and there’s been a court ruling that has actually overridden those rights.
So it’s not impossible to override them. The ministry doesn’t say it wants to override consu, just objection. But the way that it is framing its proposed changes is that if you are a doctor and you’ve got a patient who wants euthanasia, then you need to assist them in accessing it. So that means.
Providing you know, results, reports, stuff that, that would go into their paperwork and pointing them in the direction of someone who can perform it. Very few doctors perform euthanasia. There’s only a handful on the registered list, so it’s not like they know that not all doctors are going to participate in it.
Actively, but conscientious objection, rights. Acknowledge that by helping someone do something that you think is not in their best interest. It’s called moral injury. When you believe one thing, but you are compelled to do something else. And as a professional whose job is to care for people, that’s a really serious thing to put on someone.
So they’re not saying you have to be the one. Doing the injection, but they are saying we think that there shouldn’t be room for a doctor to step back and go, you know, there’s a national number you can call, you can get information there and then you know, wash their hands of it, which would allow a doctor to go, okay, I’m not aiding and abetting something that I actually think is not in this person’s best interest.
Simon: So why do you think they’re trying to fall? I mean, again, this is only a suggestion from the Ministry of Health. You, right. Again, touching on Canada is a very worrying example. I mean, we’ve held the right of conscience is one of our fundamental rights for a long time. Why do you think the ministry is so determined?
And that’s my word, but determined to, to remove conscience rights in this space? Knowing full well there will be that moral injury that you talk about.
Maryanne: Yeah, reading the report the wording that comes through it clearly paints a picture of their attitude is this is a consumer rights issue.
Healthcare is, we are consumers. Healthcare is something that is provided by the state. And words like patient, you know, and caregiver are absent. It is about a consumer, right? And so. In their framework, which is not a moral framework, it this is a government agency and they see if something is legal, then it is automatically good.
And if somebody wants something as a consumer, they should get it. Both of us heard Megan Vest the other week. She’s a palliative care expert and an ethicist from Australia. And so she’s been part of discussions there, as most states have legalized it. And one of the things that she highlighted, and it goes beyond euthanasia, but in, in the medical system at large, is this materialism, seeing our bodies like machines.
We’re just, you know. Bunch of components, and then you’ve got the doctors treating the broken machine and their machines themselves, they’re there to treat the patient and what the patient wants as a consumer is automatically good and right if it’s legal. And so you must do what they want. And it, it removes the complexity of going, actually we are integrated beings.
We’re mindbody and soul. And so we can’t look at it as simply as. Is it legal? Then a doctor should be fine with it and they can do it because we’re talking about ending someone’s life. This isn’t And it serious. I’m serious, doctor. Yeah. But because there’s no, no ethical kind of tearing of things. One option is as good as another is as good as another, and it just comes down to, you know, really obvious questions.
Like, like expense. Like what does the patient want? Now the added problem with that is there are not equal choices because not everybody has access to palliative care, which is the obvious good option for people who are suffering at their end of their life, who are terminal and who need pain relief and symptom control, and help walking through this.
This end of life stage because it’s not just about, oh, you’re gonna die and then you die there, there is an actual process and to die, well, it involves other people because we’re in a relationship with other people and those relationships are gonna end. It involves growing the way we do in every other stage of our life.
I mean, suffering is a part of life. And to say, well, we just need to take away the suffering, and then everything is fine. Well, you’re taking away the life as well. So there are questions around this. The ministry’s review doesn’t go and doesn’t touch on any of this complexity. It keeps it very simple and goes, if the patient wants it, they should get it.
The doctor’s there to provide a service.
Simon: It’s almost not a doctor then I would argue, I mean, I expect I better personalize it. Because you might have a different view and certainly others might is, you know, we want doctors to bring their whole self. So of course their medical knowledge, their training, their scientific understanding.
But we also want their empathy, their humanity, their ethics. And it worries me when we have. And we see this across a number of the medical ethical issues. Yeah. Doctors are just being reduced to functionaries, as you say, to machines. I think that should concern people because we expect more of our doctors.
And if these recommendations were to go ahead. I mean, from your research and your thinking, we’d probably see a number of doctors and nurses actually leave the profession that, that this would be a line they don’t want to cross.
Maryanne: Yeah. And this is something that the ministry should be addressing because even if it doesn’t want to weigh into ethical and moral matters, it needs to be aware of practical ones.
So when there’s one hospice in New Zealand that when euthanasia became legal, so yeah, will offer it here, only one. Hospice New Zealand Palliative Care Specialists, by and large do not think that euthanasia. Is necessary. The one that did, I had somebody who worked there tell me that they lost their lead nurse and a whole bunch of their staff, like over a dozen staff.
Medical staff left when they started offering euthanasia because those people didn’t want to work in an environment where people’s lives were being actively ended. They’re palliative care specialists now. This is one thing that, that Megan brought up. There has been a study done. This is back in 2016, journal of Contraception and Reproductive Healthcare.
The title of the journal article is, yes, we Can Successful Examples of Disallowing, conscientious Objection and Reproductive Healthcare. So this is dealing with abortion and they’re the way they address the problem of, well, some people who go into this field. Won’t want to participate is those people are able to find work in another field of medicine.
Not a problem, just they can work elsewhere if they’re not happy with it. But this is what it involves. Instead of recognizing that you are putting people under pressure, even if they don’t leave the field, there are a lot of people who don’t want to be participating in that. Conscientious rights have to be protected or you will lose people.
And already this event the other day. Just anecdotally, there are people talking about health. They have recognized that there are fewer people training for beginning of life stuff because they don’t want to be compromised. And there are people choosing not to you know, specialize in palliative care.
There are fewer and fewer palliative care specialists. And given the change in law there’s probably connection for some of them in that as well. They do not want to go into. A profession where lives are going to be actively ended, even if it’s somebody’s choice. Now, this is a field where we already have fewer than half as many palliative care specialists as we need in New Zealand.
We don’t want to be saying, well, they can just, they can work elsewhere. We don’t have enough to care for all of us. All are going to die. About 90% of us will be eligible for the kind of care that auspices offer. Do we want to drive people away from that profession? By saying we, we are going to mandate something that doesn’t need to be mandated.
Simon: I would argue that this shows it’s ideological the drive to actually force good doctors and nurses out of the profession in this case because they won’t practice euthanasia. And the same as actually in the abortion space is, yeah. The strongest signal that we’re dealing with an ideological drive here.
It’s not practical. It’s not feasible, it’s not economically sensible. But it’s ideological. There, there can be no resistance and it seems to me, Maryanne, the more radical the ethical issue is, the more the ideological drive to, again, force. People out. And I would make the argument, the Ministry of Health seems willing to accept that because their review, as far as I was reading, I didn’t pick up anything in there saying, oh, well if we remove conscience rights from doctors and nurses, they’ll leave.
Or some will leave in a system already under pressure.
Maryanne: Yeah. And you mentioned Care Homes they would like, and this is not currently legal at the moment, care Homes can choose whether or not they offer it on site. The ministry would like that to change again, to for ease of access so that if a care home doesn’t allow it onsite, they lose their registration.
I mean, that’s very heavy handed.
Simon: Oh, massively. So is a heavy handed, can you imagine
Maryanne: like taking hospices offline because. They won’t allow it on site. I mean, people can still access euthanasia, not in a care home. That might be their first choice. But there are lots of things that we want and don’t get because it’s not convenient to other people.
And so if people don’t want to live in a care home where people are being euthanized next door they shouldn’t have to. And it’s perfectly reasonable. In fact, the report said one of the options they considered is that. Care homes have to be upfront when people move in and say, look, we don’t provide euthanasia on site.
If you want to access that, you have to go elsewhere. And then let the person, the consumer, make the choice. And they disregarded that because it would limit access. So they said, we can’t do that.
Simon: I personally find it extraordinary, particularly in the autonomy. Argument or space in so far as if it’s an autonomous choice or rather one exercises their autonomy to choose euthanasia or assisted suicide.
Why is autonomy, if you will, or freedom not being given to the care homes, to hospices, to, to doctors their autonomy has been, or proposed to be aggressively removed? And I’m pleased you, you bring up the care homes. Yeah. If they. They could be shut down. I mean, that is an exceptionally yeah.
Aggressive move.
Maryanne: Yeah. And this is what, well, whoever’s writing it from the ministry I don’t, I don’t know what the balance of opinion is, but those who are behind the review, that’s their opinion. Yeah.
Simon: It’s just, again, the strong army and anti autonomy this is what I, well and anti
Maryanne: choice. One of the things I highlight here is not everybody has access to palliative care or hospices, which is by far the best option at end of life for anyone.
And there may be people, exceptions you can point to and go have an a, a legitimate argument about well would. Would euthanasia be more merciful because this person is suffering horribly and all the rest? And that’s another debate. But what you can’t debate is that palliative care is the best thing hands down for people at the end of their lives.
You don’t know. Suddenly it is keeping symptoms in check. It’s managing like these people are. Experts in managing pain. They counsel people as to, you know, the process, what to expect. So that eases people’s anxiety. They know what’s coming, and it brings the whole whanau in so people around them understand what’s going on.
Everybody is coached through something that’s quite foreign and scary to us. I mean, who, what else would you want? Not everybody has access to it. It’s not fully funded. So you’ve got people who, because euthanasia is fully funded, can access euthanasia and can’t access palliative care, that’s not great choice.
Simon: I think that’s something that needs to be and why. I really like your discussion payer. Because it drives that home. If you want to have a choice argument, and this is me. Paraphrasing if those who want to pursue the choice or the autonomy argument then palliative care needs to be an actual choice, which it isn’t for many.
I don’t have the numbers in front of me, but you know your paper better than I do. Seeing you wrote it, you had some percentages statistics around actually how many New Zealanders can access palliative care and it’s woefully low.
Maryanne: Yeah, and it’s really hard to get an exact number because it’s not like you definitely have it here.
You don’t here for children, Starship is the only place that offers paediatric palliative care. So if you’re outside of Auckland then that kind of care gets kind of patched together. And so if you find somebody who’s, oh, look at me, I think I’m doing thumbs down. If you find somebody sit hands.
Who is willing to offer?
Simon: No, I was just saying idea. I muted myself. It’s one of my big mis I was just saying it just brings a little bit of levity into what’s actually a a heavy topic.
Maryanne: I know. Otherwise we would not be smiling at all. Yeah, and the paediatric palliative care is a little bit. Tragic because that I mean, children do suffer from terminal illnesses and die.
And if you’re outside of the Auckland region, there’ve been some mainstream media has picked up some of these stories and it’s been really good. To highlight the fact that parents of kids outside of Auckland are really stuck if their kids are deteriorating because you have to find somebody who has the skills, who’s willing to treat them, and some people just can’t.
So it’s just patched together. Absolute numbers is really difficult to come up with. Roughly we have roughly half the number of specialists. Of those who died last year, about a third of those who would be eligible for hospice care accessed it. Some of those would’ve accessed specialized palliative care in a hospital.
Some might’ve accessed it some other way, but we’re rough. We roughly need twice as many easily as we currently have, and the number’s only going to increase, and we have. The line for palliative care specialists is going down and the line for demand is going up.
Simon: And as we have an aging population, I mean, obviously, you know, palliative care is not strictly linked to age, but obviously more people who are older people and approaching end of life need it. I mean, it’s almost scandalous. I would argue and I was talking to Tanya Kovich recently. She’s an MP who’s picked up a bill that myself and before that Maggie Barry had saying that we need to not only fund palliative care, but actually have a plan.
There isn’t even a palliative care plan around the country. And I think what really. Highlights. The problem in linking it even to the question of euthanasia is the review panel or review committee of the End of Life Choice Act. There are three people, as you know, they were noting access to palliative care in the rural areas was, well, it’s almost non-existent.
And that they had sort of a worrying concern, Maryanne, that. People were then seeking, more people in the rural areas were seeking euthanasia because they didn’t have access and the ministry blocked them from the necessary data to actually confirm or otherwise that suspicion. Yeah,
Maryanne: I didn’t know that bill was originally yours in Maggie’s before that.
I’m so pleased that Tanya has this bill in there and she’s made it better. I didn’t know what it before, but. It is just astounding that we can emphasize choice but not emphasize fully funding palliative care. So I’m really glad that bill’s in there. I hope it gets pulled and I hope there’s a discussion about it because there needs to be the level of commitment that the ministry has to making sure everybody connects as euthanasia should be the level of commitment there is to making sure everybody can access palliative care and it’s not there.
Simon: No. And we’re seeing from overseas jurisdictions that people end up, well euthanasia is seen as the easy, cheaper way out. Yeah, if you Yeah. Which is deeply worrying. And actually that leads me, your paper also talks about the recommendation, again, from the Ministry of Health to allow doctors to talk about euthanasia to patients.
At the moment, they’re not really allowed to seed the idea. I mean, talk us through why. You know, for some people going, well, why wouldn’t the doctor talk to me about this as an option in the same way they can give me pharmaceutical options? So what’s the issue here?
Maryanne: Yeah. And even though the legislation says they mustn’t, some do the reason the simplest way I can put it is if you’re going to a doctor for medical problem and you’re under stress already because you’re facing this challenge, and they say, have you considered euthanasia?
What is that going to do to your will to look into your treatment options? I mean, it just completely decimate the kind of hope that you need to face a challenge like that. And when it’s a doctor saying it, I mean, it’s bad enough when it’s somebody’s child or something, because then that puts the thought in somebody’s head, oh, if they think this is what’s best for me and they love me, then you know, if your doctor is saying it.
One of the stories that I I included in the paper comes from Dr. Katherine men’s. Book with the end in mind. She tells story after story af you know, she spent decades in palliative care and she shares individual stories and it illustrates how different personalities, different health problems and needs can be met in different ways.
One of the people she treated had been in the Netherlands young dad. The terminal, I think it was cancer and every ward round. Because he needed constant care for treatment manage to manage his symptoms. Every ward round somebody would bring up euthanasia with him. Because you know, the Netherlands, they’ve got very loose restrictions around it, and it’s been common for a while and it made him feel guilty.
He said he was dreading ward rounds because he knew that there would be this conversation again, and he knew that. By not taking it. He could be. Being a burden on his family. He felt like he was a coward for not taking it. Like there were all these, it wasn’t just a choice it was a burden for him. He literally ran away to the UK.
He had family in the UK. He went there with his wife and his daughter and spent two former peaceful months. In palliative care being cared for by Katherine Maddox, and when he did die, he slipped into a coma. His daughter was playing outside. It was peaceful. It was the kind of death that people would say they want.
It wasn’t with the stresses of the decisions and the pressure from the health system saying, well. Because at the end of the day, as soon as somebody raises euthanasia with you, having looked at your prognosis, and they say, have you considered this? There’s nothing else to read between the lines, but you may be better off debt.
Simon: Yeah. And a person in authority in this case. Yeah. And it’s one of the reasons why euthanasia advocates have always wanted doctors to do the terminations. I would suggest, because it gives the white coat of legitimacy. You know, I certainly raised it when I was on the select committee that, you know, it’s not actually, and I’m not going to go into the specifics, but actually it’s not that difficult.
The process that is used to kill someone, you don’t have to be a doctor, but of course, doctors give a legitimacy and they hold an enormous amount of. Power. Which I find is ironic for, again, those on the more progressive side of politics who push this. Because they’re always about power and hierarchy and you go, well actually having your doctor tell you that euthanasia is an option, legitimizes it seeds the idea.
And yeah, because it’s the doctor telling you, you go, well, maybe that is the right option. In the same way when the doc says to me, we’re going to give you these pills, I don’t question it usually. Okay, doc. Thanks very much.
Maryanne: Yeah. Yeah. And it, it is part of what we were talking about before. It’s not just putting an option on the table, it’s normalizing it.
If you wouldn’t mind me reading a section of the paper that I think I’m quoting some of the ministry’s review here and what it highlights is that it isn’t enough for it to be available. It needs to be accepted from their perspective. So I’m saying the Ministry of Health does not acknowledge that there are valid reasons to opt out of participating in euthanasia.
It identifies that quote, and this is from the review. Some communities, tikanga custom values are not aligned with or supportive of assisted dying and that some held the view that the UA spirit belongs to God and the body should be allowed to perish naturally. End quote. I say this belief shared not just by many Māori, but also by many faith communities, is one that the ministry considers misguided regarding mana, who consider euthanasia to be the same as suicide.
They write, quote, this is the ministry that this points to a lack of awareness and acceptability of assisted dying within our communities, and an urgent need for assisted dying to become familiar, understood, and accepted.
Simon: So we’re going to expect I’m being a bit facetious here but you know, are we going to expect to see struggle sessions from the Ministry of Health onto people that you all have to change your views.
You’ve got to come to understand that our take on euthanasia’s, right? I mean, that’s chilling. I have to say actually, Marianne.
Maryanne: Yeah, I mean, it’s legal, so it’s right. It’s as simple as that from their perspective. And so anybody who sees ethical or even practical problems with it will not have any sympathy from the ministry, which, if you’re a doctor working in that system is really hard.
Simon: Well, again it. I suppose my former political hat on, and even my philosophical one, it’s a deeply worrying dynamic because their view is, okay, there are differences of opinion. We’re not going to debate or discuss them. You are just going to have to change. You know, you’re just wrong. We are right. And we will use all the conversive power of the state including sacking you to make sure you understand.
I mean, it’s it, or understand the view as they, they have it. And again, all of this in the argument of autonomy and choice. Again I, yeah. Can never fathom Maryanne, how these guys cannot see the hypocrisy to be honest in their position, but it just deeply ideological.
Maryanne: Just and sorry.
I was just going to say, digging into that word choices, I mean, some of what I go into is just unpacking this idea of our choices being somehow sacred, when actually we change our minds all the time. So the fact that there isn’t a cool down period to consider this highlights the limitations on choice because actually good choice.
You, you take things into consideration when you’ve been given a terminal diagnosis and you’re in unchartered territory. You are not at your best when it comes to decision making. You would think that having a cool down period and. Have to see a psychiatrist, which now is only for people where there’s doubts about mental capacity and even then it’s just to make sure that somebody is competent to ascent.
It’s not to say, do you need some counselling? Do you need some help? This is a tough time you’re going through. That is not embedded in their framework for choice. It is entirely around expediting the process. The fastest time so far from application to death is two days.
Simon: Two days. Beause they make a big thing of it.
Sort of The average I think is 16 if memory serves me right. And feel free to, it depends. Two days
Maryanne: it depends. Yeah, like me mean median mode. There are some outliers at the upper end. So there published average is around three weeks, but actually the most common timeframe is two weeks. And yeah, two days.
I, I don’t see how that serves someone’s choices, you know, allowing it to happen that quickly, especially when, how can you check that there’s been no coercion and approve it and receive euthanasia in two days? I, the safeguards are on coercion. They’re there on paper. But when you look at what’s been going on and when you hear the testimony of two of the original three review committee members, you recognize.
That there are no safeguards against coercion. It’s what we don’t know can’t hurt us.
Simon: There are no safeguards at all. I actually, it’s been one of the things, one of my little drums I keep beating or ranting on my little soapboxes. There is no safeguards in the law. There’s a whole series of processes.
Yeah. Tick boxes. Yeah.
Maryanne: Yeah. Well, and when the tick boxes were blank the review committee members found that. There was information missing, and when they brought that to the ministry’s attention, the ministry said, I assume nothing’s wrong. If there’s no information. They’re the review committee if.
They are reviewing it, finding something missing, and then being told like with the higher numbers of rural applicants, and if they’re being told, oh, don’t worry about it. Well, what is a review committee for if they’re not to review it? They found that there was one person who’d been euthanized, who didn’t speak English, didn’t have an interpreter with them when they were having the consultation and was suspected of having dementia.How did that happen? And they didn’t get any answers.
Simon: No. And I think is one of the many reasons why effectively, I think one resigned from the review committee and the other who was raising questions did not have her time renewed. I. Because it was, yeah, inconvenience, and it wasn’t the word that I had in my mind when we started this chat, although I’ve used it a few times.
It’s ideology and I just can’t help feel we have ideological zealots. Again my opinion within the ministry pushing this because they believe it’s just normal healthcare. Just like going and getting, as I say, some neuro fend for your headache. This is just normal. Hence why they can’t tolerate.
Questions they can’t tolerate, actually people pushing back and why they want to snuff out the likes of conscience rights. This is deeply driven and it’s not medical or scientific, I would argue this approach. It’s not standing up to scrutiny.
Maryanne: No, because they would be taking, you know, the concerns of the review committee, for instance, seriously, they would be taking seriously the impact on staffing.
Like those are things that would be considered if this was balanced. But everything is driven by the fundamental need for quick and easy access throughout the whole review. That was the bottom line.
Simon: Which I’ve always found ironic. I mean, don’t get me wrong, we don’t, you know, in the broad sense, obviously I’m opposed to euthanasia conceptually, but it’s, you know, you don’t want people to be unnecessarily burdened.
But actually the current situation, I said it’s fully funded. There are few doctors, but enough of them, and I’ve always been struck Maryanne, that if you are a person deciding to end there. They’re alive and you’ve made all those, I don’t know, choices. You, you can, you know, travel just that little bit further if you need or wait just that little bit longer.
You know, this is an enormous decision and yet somehow the final steps have to be so easy, simple, and accessible, that ethical principles, things like conscience rights are just going to be tossed out the window.
Maryanne: Yeah.
Simon: Nutty, by the way. I’ve only just written about it in recent days, but the, this very same ministry of Health and I feel like I’m bagging the entire ministry.
I, I shouldn’t be, but it’s really those who are behind this review. They can’t even count the numbers right. They’ve just updated some of their quarterly reports from last year and discovered in one quarter there were 56 more people who had died than they realized almost double the original.
Numbers. So, you know, the very ministry conducting this, again, I’ll use that word, ideological review can’t even tell us accurately how many people are being terminated. I mean, it’s just, it’s clearly ‘safeguards’ are not there or working.
Maryanne: Yeah. I saw that you guys were onto that and the sad thing is I wasn’t surprised and the.
We’re at a rate of not quite one a day. That should be pretty easy to keep track of, and this is somebody’s life ending, so it’s pretty consequential. I don’t know how they can’t keep just the basic count straight. Yeah. If they can’t do that, as you’ve pointed out, how are we trusting them to meet all these other requirements?
Simon: Well, you will know in the work to put this discussion paper together. The ministry says in its review that it’s all working perfectly. I don’t have it literally written verbatim in front of me, but in effect, they say that everything is fine working well. Yeah, and it’s like it’s demonstrably false.
We should end on a positive because of course, with all of your research and discussion. Papers In your work at Maxim, you have a variety of recommendations of how, you know New Zealand should move forward in this space. Do you want to quickly take us through those?
Maryanne: Yeah. I’ll get them in front of me so that I don’t miss any.
Simon: Yeah. It’s not a test, fortunately.
Maryanne: Yeah. So the bullet points are you’re,
Simon: as you’re pulling that together, actually, a side question, I mean, as someone who researches deeply into this space, how affecting do you find it? Obviously you’re a professional researcher, but you know, these are heavy topics. If you don’t mind me asking, how do you find it as you delve into these things?
Maryanne: I hadn’t dive deeply until kind of the end of last year. And I was pretty grumpy for a month or two. It was weird because I was reading and some of it, oh, I have book. If anybody wants an excellent book, Catherine Manix says, was the end in mind. I probably cried at Parts First Four chapter chapters and then some others.
Simon: It’s a great book. Highly recommend it.
Maryanne: Yeah, and it’s I’m making it sound like it’s sad, it’s enlightening. I feel like I understand the end of life and dying. Well, so much better. And there’s other good stuff out there as well. But she’s a genius. So reading that was a bright spot. It is just a little bit hard because you recognize that vulnerable people are made more vulnerable by the way this is being managed. And I was just, you know, reading a lot about death, which isn’t something we do all the time. But it’s good to be having these discussions and encouraging others to have these discussions.
Because I think it’s really important that we don’t just stay naive and stay ignorant because then we’re liable just to, to react emotionally. To the way things are phrased and worded and we become much more easy to manipulate instead of thinking deeply about these things.
Simon: Which is why I think the, again, the work you are leading, maxim’s leading and others in the space like Catherine’s book is so important.
And look, thanks for asking that because I know it’s a bit more. Personally, I know having for literally a couple of years when I was on the select committee and then the bill was going through Parliament at, you know, literally years of basically thinking about death and dying every day saying, oh God, I’m surprised I didn’t end up on any antidepressants or anything, but, you know.
Yeah. Tell us about your recommendations.
Maryanne: Yep. Well, the first is like we were talking about better information. I mean, our choices are dependent on the information we have and the actual options we are given. So the more we know about what a natural end of life entails, the stages our bodies go through and what options are available in the health system that’ll just improve things right away.
It’s called death literacy, providing universal access to palliative care is the second one. And I. Everybody, everybody would win if we could do that. And just encouraging people. It encouraged the system itself to be proactively training people in that area. Even other specialists can upskill in palliative care.
So that needs to happen through this prioritizing training, which I started going into. So we need the people to provide the palliative care. Hospice is obviously, yeah, just building that up and then fortifying the protections around euthanasia, and we have the most points around that because that’s really a pressing concern.
The ministry is clearly trying to remove some of those protections, and they’re not strong enough as they are.
Simon: No, it’s the irony of everything you’ve talked about all the evidence that’s actually coming forward in the public space. Anyone watching here can jump online and actually find, you know, not only of the discussion paper that Maryanne’s done, but all the problems that we’re identified and yet the pushing past those, ignoring those.
And to be fair too, it’s the politicians. So it’s not just, not just the ministry, but wanting to expand this. So it’s really good. You know, from my perspective, you talk about fortifying the position more is needed. So Maryanne, if someone wants to get hold of this paper and read it, and I highly recommend that people do.
Where do they go?
Maryanne: They go to maxim.org.nz and there’s a little tab with our research. You can also go onto the website and just sign up to receive our monthly bulletins. And anytime we put out something like this, you’ll get it
Simon: and I’d highly encourage our viewers to do so because the work that Maryanne and the team there at Maxim do is.
Fantastic. And wide ranging. But look, Marianne, very grateful for your work and research and again, you know, these are heavy topics. So grateful for you taking that time just to yeah, chat with me about them and being part of the show.
Maryanne: Thankful for you, Simon. I really appreciate it.
The excellent article “Are We Euthanising Choice?” critiques the implementation of New Zealand’s End of Life Choice Act 2019, arguing that the reality of assisted dying diverges sharply from the promise of autonomy and fairness. While the Ministry of Health claims the system is operating well, a review committee has raised concerns about missing and contradictory information in euthanasia cases. One particularly troubling example involves a non-English-speaking patient being euthanised without a translator present, and had likely suffered from dementia.
ACT wants to expand euthanasia but this would breach fundamental human rights in the New Zealand Bill of Rights Act.
“ACT’s changes breach human rights and take away freedom of choice,” says Alex Penk, author of a new report for MPs on the End of Life Choice Amendment Bill. “The Bill would stop doctors and care facilities like hospices from using their conscience and making ethical decisions like they do now.”
“Assisted dying is already highly controversial and most doctors don’t want to be involved,” says Penk. “The Bill would introduce euthanasia for long-term conditions and disabilities, like chronic heart conditions, frailty, diabetes, renal failure, multiple sclerosis, and motor neurone disease. This would force doctors and care facilities into more conscience conflicts. Doctors have to use ethical judgment all the time but the Bill sends a message that they’re just supposed to do what the state tells them. There’s a real risk it’ll force ethically-minded people out of medicine.”
“ACT’s bill would also undermine palliative care. It would cover ‘care facilities’, including hospices, disability support facilities, and rest homes. Care facilities would have to be prepared to allow assisted dying even when that goes against their beliefs. Facilities like hospices do an incredible job for vulnerable people but they’re over-stretched and under-funded. They shouldn’t be backed into a corner if they don’t want to be involved in euthanising their residents.”
“This is not what Kiwis voted for,” says Mr Penk. “David Seymour said that conscience is a cornerstone of the law, and 65 percent of voters supported that law in a referendum. There is no mandate to change such a fundamental part of the law. Let individual doctors and care facilities decide if they want to offer assisted dying, or the government could just do a better job of providing information.”
“It’s ironic that a law about end-of-life choice would limit freedom of choice,” says Penk. “MPs will get a conscience vote if the Bill goes before Parliament. Why shouldn’t doctors and care facilities get to use their conscience too?”
A US film about assisted dying and the treatment of people with disabilities is set to premiere at this year’s Sundance Film Festival. Titled “Life After”, the feature documentary by Reid Davenport (who also has cerebral palsy) explores the story of Elizabeth Bouvia, a 26-year-old woman with cerebral palsy and arthritis, who in 1983 attempted to starve herself to death in a California hospital, citing that life wasn’t worth living. The legal battle that followed turned her into a public figure. A court ruled she did not have the right to die.
However, in 1986, a judge reversed the decision, but Bouvia chose to continue living, though she still preferred to die under different circumstances. She later lived with a live-in nurse in her own apartment until her death in 2014.
The filmmaker also heads to Canada to explore one of the world’s most aggressive assisted dying programs known as MAID (medical assistance in dying). Canada’s Medical Assistance in Dying (MAID) program, which allows euthanasia for chronic illnesses or disabilities, has increased, and MAID is now the 5th leading cause of Canadian deaths. Davenport digs into the unprecedented rise in disabled people dying prematurely due to MAID and speaks to advocates, patients and doctors who believe euthanasia saves healthcare costs. Davenport views this as a troubling factor in the rise of euthanasia. Davenport acknowledges that assisted dying, in theory, could be safe for terminally ill adults but believes it’s unsafe and risky in a neoliberal society where patients face significant social and economic pressures. Davenport worries that society encourages people with disabilities or chronic medical conditions to view life as not worth living.
The film director is cautious about his documentary being seen as cynical or alarmist by pro-euthanasia advocates and progressives. Davenport believes the issue of assisted dying is complex and that disability activists, not just conservatives, have valid concerns about the potential for abuse and the “slippery slope” argument. He notes that even if the slippery slope argument is seen as fear-mongering, there are instances where it is valid.
The film in varying confronts two powerful systems—the healthcare and bureaucratic systems—challenging their responsibility for overlooking how their shortcomings and policies may not be as effective as they seem. More importantly, Life After is a crucial exploration of the value of life itself.
The push to pass euthanasia and physician-assisted suicide laws over the past few years has seen a global rise and acceleration of various jurisdictions legalising and normalising assisted suicide. New Zealand, Austria, and Spain all legalized it in 2021, with parts of Australia doing the same in 2022. In Italy, the first assisted suicide took place in 2022. And most recently, the United Kingdom, in late November last year, took the first step in passing a physician-assisted suicide measure that would open the door to the practice of allowing doctors to help people take their own lives.
France, Scotland, and Ireland are contemplating similar measures, as well as 19 other jurisdictions that have some form of physician-assisted suicide on the books. In the USA, 10 states and the District of Columbia have legislated physician-assisted suicide, with other states like Delaware, New York, and Maryland looking to secure similar laws.
In countries like Belgium and the Netherlands, where physician-assisted suicide has been legal for more than 10 years (in Belgium and the Netherlands since 2002), those eligible for death by a physician are not just the terminally ill, but those with “chronic, nonterminal, or treatment-refractory illness,” with treatment-refractory illnesses being those conditions that do not respond to treatment. Off growing concern is Canada, which has the most aggressive assisted suicide laws where MAID (medical assistance in dying) is now the fifth leading cause of Canadian deaths and access to MAID services are no longer confined to the terminally ill but can also apply to individuals who are homeless, feeling lonely after the death of a loved one or/and in despair.
In a day and age where there is a growing epidemic of loneliness and despair, we should not be encouraging a culture of death as the antidote to life and its challenges.